Page 38 - 1. kongres program
P. 38
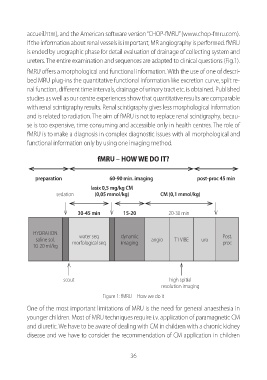
accueil.htm), and the American software version “CHOP-fMRU” (www.chop-fmru.com). If the information about renal vessels is important, MR angiography is performed. fMRU is ended by urographic phase for detail evaluation of drainage of collecting system and ureters. The entire examination and sequences are adapted to clinical questions (Fig.1). fMRU offers a morphological and functional information. With the use of one of descri- bed MRU plug-ins the quantitative functional information like excretion curve, split re- nal function, different time intervals, drainage of urinary tract etc. is obtained. Published studies as well as our centre experiences show that quantitative results are comparable with renal scintigraphy results. Renal scintigraphy gives less morphological information and is related to radiation. The aim of fMRU is not to replace renal scintigraphy, becau- se is too expensive, time consuming and accessible only in health centres. The role of fMRU is to make a diagnosis in complex diagnostic issues with all morphological and functional information only by using one imaging method. fmrU – How we do it? preparation 60-90 min. imaging post-proc 45 min lasix 0,5 mg/kg CM sedation (0,05 mmol/kg) CM (0,1 mmol/kg) 30-45 min 15-20 20-30 min HYDRATION water seq dynamic Post. saline sol. angio T1 VIBE uro 10-20 ml/kg morfological seq imaging proc scout high spitial resolution imaging Figure 1: fMRU – How we do it One of the most important limitations of MRU is the need for general anaesthesia in younger children. Most of MRU techniques require i.v. application of paramagnetic CM and diuretic. We have to be aware of dealing with CM in children with a chronic kidney disease and we have to consider the recommendation of CM application in children 36